
By Usama Jamil
15 min read
AI in Radiology: Why It's Becoming Part of Everyday Practice
Why AI in Radiology Is No Longer Optional
Radiology has always been one of medicine's most data-intensive disciplines. A single CT scan of the chest can generate over a thousand images. A busy hospital reads tens of thousands of studies every year. And the radiologist interpreting those scans is expected to be fast, accurate, and consistently alert, often across long shifts, on-call overnight, and under growing administrative pressure.
That structural strain is real, and it is getting worse. The U.S. faces a projected shortage of 17,000 to 42,000 radiologists, pathologists, and psychiatrists by 2033, according to the Association of American Medical Colleges (AAMC). Between 2008 and 2019, workloads for practicing radiologists increased by 80% while the time residents dedicated to radiology training declined by 25%. Burnout rates now sit between 51% and 54%, making radiology one of the specialties most affected by workload pressure, according to RSNA. And yet imaging volumes keep climbing, driven by an aging population, rising rates of chronic disease, and the expanding role of imaging in treatment planning.
AI did not create this problem. But AI in radiology is increasingly the most credible tool for addressing it.
This is not about replacing radiologists. That framing misses what is actually happening. The better question is what radiology AI can take off a radiologist's plate, the high-volume, repetitive pattern recognition that drains attention, while leaving the clinical judgment, contextual reasoning, and patient accountability where it belongs: with the clinician.
The Numbers Behind Radiology AI Adoption
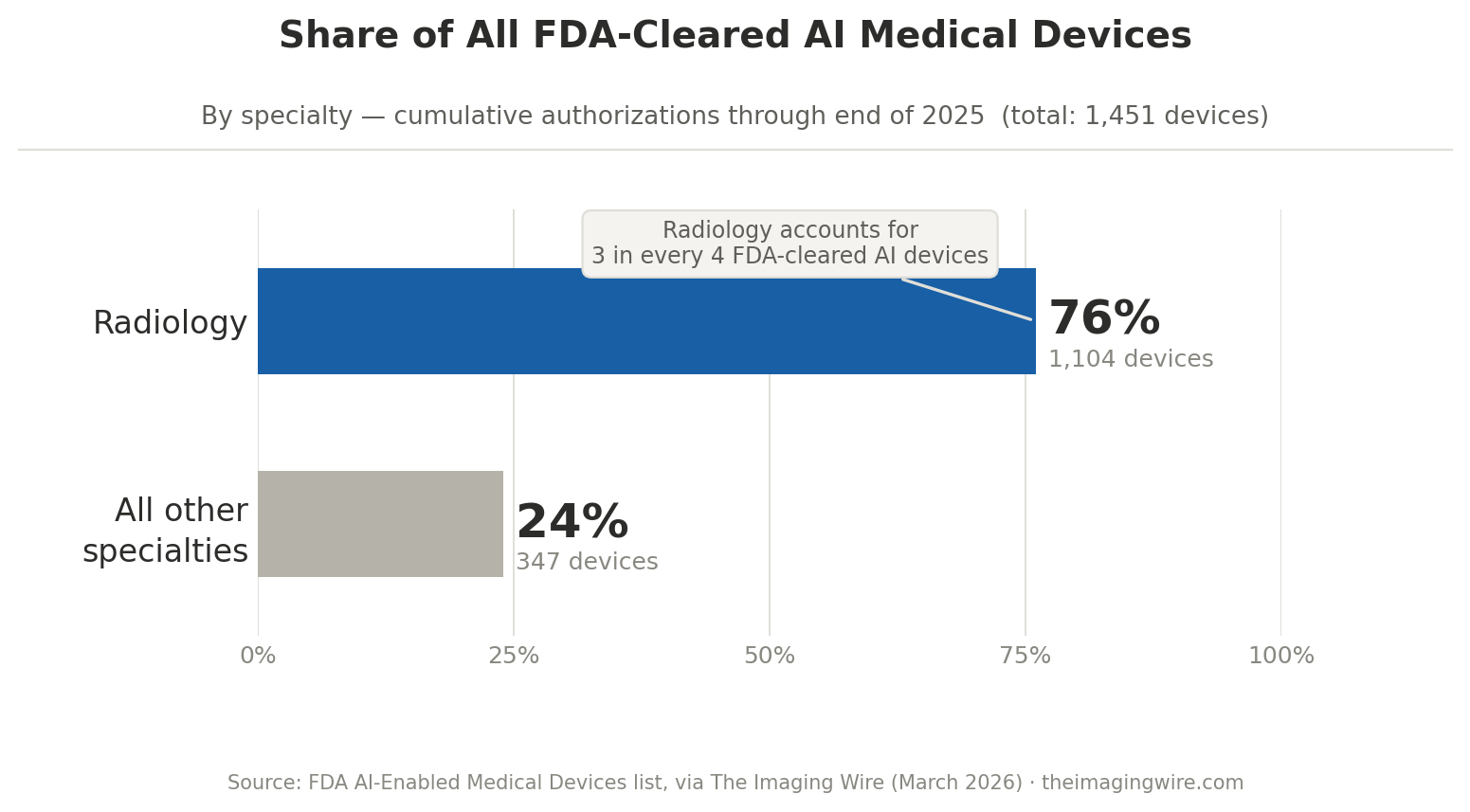
One of the clearest indicators of how seriously the field has moved is the FDA's own authorization list. As of the end of 2025, the agency had authorized 1,451 AI-enabled medical devices. Of those, 1,104 — 76% — were radiology devices. In the fourth quarter of 2025 alone, 55 of 72 newly cleared AI devices were designed for radiology. The FDA publishes a continuously updated list of AI/ML-enabled medical devices that has become the de facto reference point for the field.
This does not mean every device on that list has strong clinical evidence behind it. A 2025 JAMA systematic review found that only 5% of healthcare AI studies used real patient care data for evaluation, and most approved devices were cleared via the 510(k) pathway, which allows market entry by demonstrating equivalence to a previous device rather than independent clinical proof of performance. That is an important distinction, and a real limitation to keep in mind.
But the direction is unmistakable. Radiology is where AI in medicine is most mature, most tested, and most actively deployed.
What AI in Radiology Can Actually Do Today
The earliest and most credible wins in radiology AI are in detection and triage — tasks where the cost of missing something is high and the signal is visually structured enough that deep learning models can be trained effectively.
AI in chest CT and pulmonary imaging
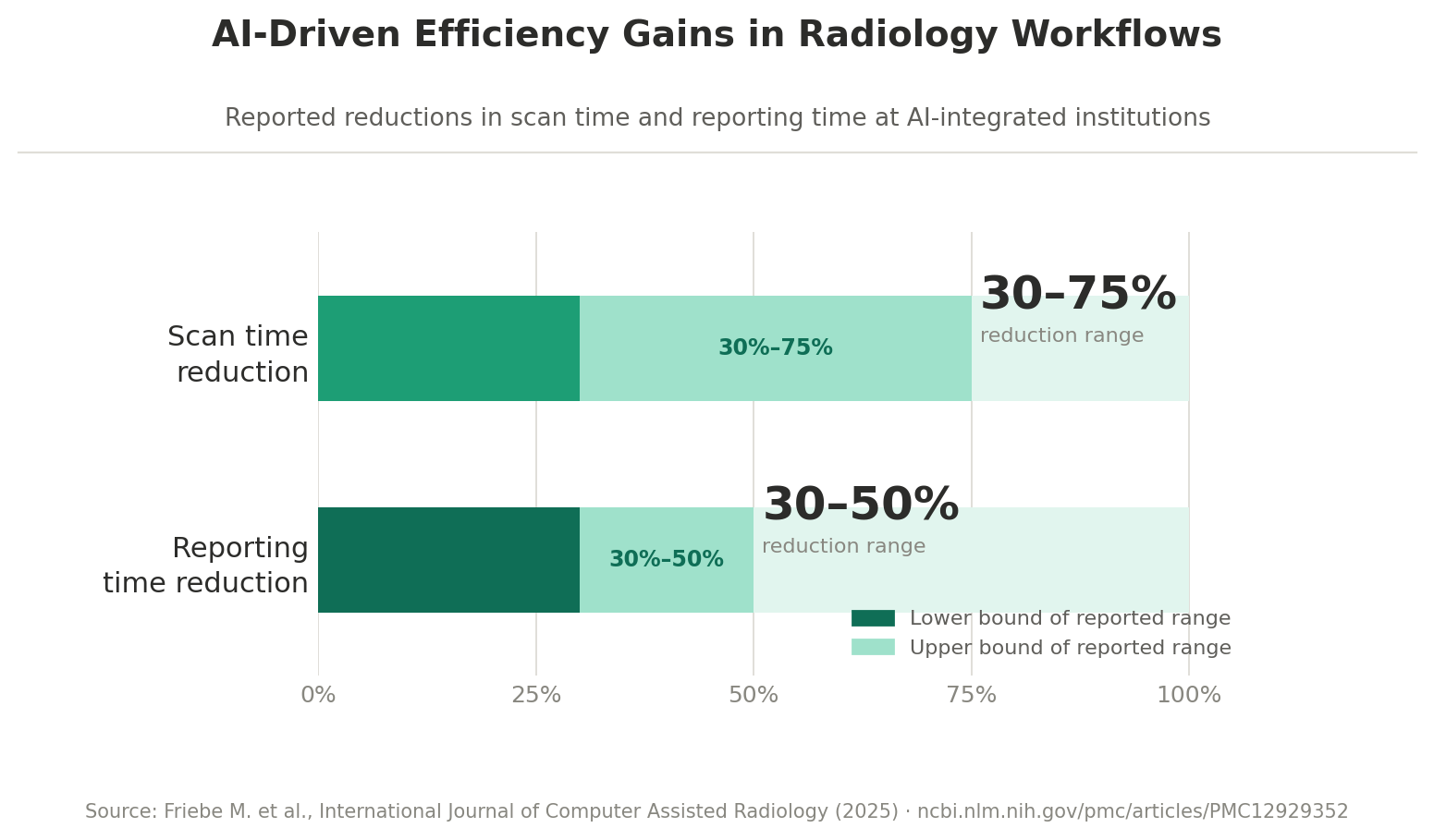
In chest CT, AI systems now achieve nodule detection sensitivity of up to 95% and segmentation accuracy of up to 94%, according to a 2025 structured narrative review published in a peer-reviewed journal on computer-assisted interventions. Scan time reductions of 30–75% have been reported in certain imaging workflows, alongside 30–50% faster reporting times in institutions that have embedded AI directly into their PACS and reading workflows.
In neuroimaging, deep learning models have demonstrated an AUC of 93.2% in distinguishing between low-grade and high-grade gliomas using MRI data — results that, in some studies, outperform traditional diagnostic approaches in specific classification tasks. In mammography, MRI, and ultrasound for breast disease, AUC ranges between 0.868 and 0.909 have been demonstrated across large meta-analyses.
AI in breast cancer screening
In one of the most consequential recent studies, published in Nature Cancer through a collaboration between Google Research, Imperial College London, and the UK's National Health Service, an AI system identified 25% of interval breast cancers that had been missed by traditional screening. These are cases that typically surface between scheduled screenings after symptoms appear. Finding them earlier changes outcomes materially.
These are not demo results. They are appearing in peer-reviewed literature indexed on PubMed, validated on real imaging datasets, with clinical follow-through.
The Gap Between Benchmark and Production Reliability
There is an important distinction that the field has not always been honest about: benchmark performance is not the same as production reliability.
A model that achieves high AUC on a curated test dataset from a single institution is not guaranteed to generalize across scanner manufacturers, patient demographics, imaging protocols, or the ambient noise of a real clinical environment. Generalizability, calibration, and bias remain areas where the evidence base is thinner than the headline numbers suggest, as documented in post-market surveillance recommendations from the European Society of Radiology.
A 2025 review of AI in radiology found that diagnostic imaging showed higher AI maturity than interventional workflows, with 70% of MRI steps and 64% of CT steps having available AI solutions — but interventional applications still require significant human oversight. The assumption that a cleared device will perform consistently in every clinical setting is one that deployment experience has already challenged.
This is not an argument against deploying radiology AI. It is an argument for deploying it correctly.
The systems that are working in production share a few characteristics. They are scoped to specific tasks rather than general clinical judgment. They integrate into existing reading workflows rather than requiring separate interfaces, in line with RSNA's Integrating the Healthcare Enterprise (IHE) profiles. They keep a radiologist in the loop, either as a reviewer of AI-flagged findings or as the final interpreter of AI-assisted reports. And they are monitored over time, with clear mechanisms for catching drift or demographic inconsistency.
That is not a limitation. It is a design principle.
Where Radiology AI Workflow Relief Is Actually Coming From
Ask radiologists where AI in radiology is actually changing their day, and the answers are usually quieter than the headlines.
Worklist prioritization for time-critical findings
Prioritization tools that push critical findings — suspected pulmonary embolism, intracranial hemorrhage, aortic dissection — to the top of the worklist have measurably reduced time-to-read for time-sensitive cases in many institutions. In a specialty where an hour can determine whether a stroke patient receives treatment within the therapeutic window, that matters.
Automated measurements and structured reporting
Automated measurements and structured reporting tools are reducing the cognitive load of routine documentation. Instead of manually calculating nodule dimensions, tracking lesion change over time, or populating structured fields from scratch, radiologists review pre-populated outputs and focus attention on the cases that require interpretive judgment.
Teleradiology and AI-assisted preliminary reads
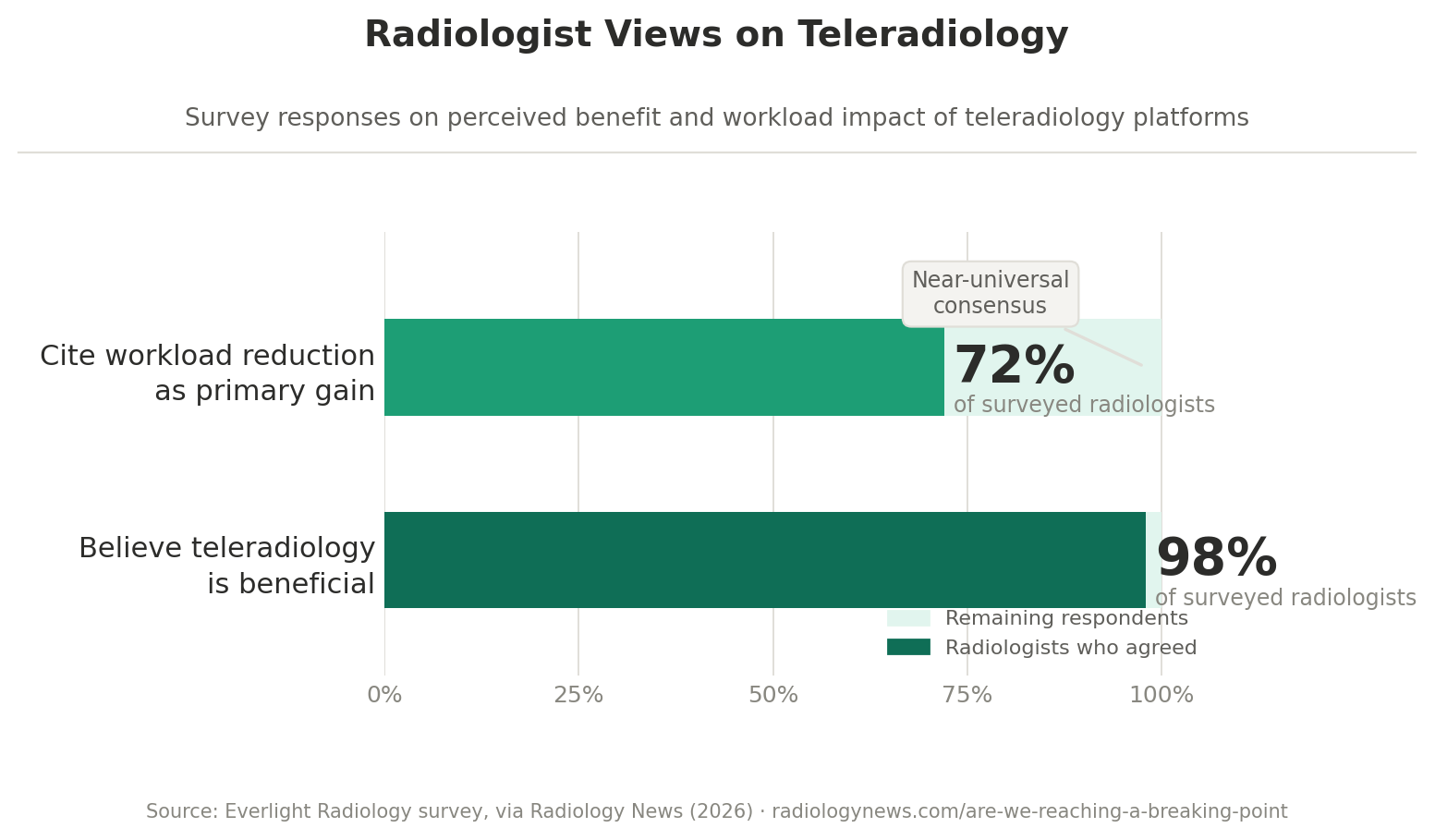
Teleradiology platforms are also increasingly central to coverage strategies, with 98% of surveyed radiologists believing teleradiology is beneficial and 72% citing workload reduction as the primary gain. AI-generated preliminary reads that a radiologist reviews and signs off on are helping smaller practices manage overnight and weekend coverage without the same level of subspecialist access.
The Rise of Multimodal Imaging AI
One of the most significant shifts in the last two years is the move from single-task models to multimodal AI systems that can reason across imaging types, clinical notes, and patient history simultaneously.
Early radiology AI was largely modality-specific: one model for chest X-ray, another for brain MRI, another for mammography. That architecture made training tractable but limited clinical utility. A radiologist does not read a CT scan in isolation — they read it in the context of the patient's history, prior imaging, lab values, and the clinical question being asked.
Foundation models trained on large, diverse datasets are beginning to close that gap. Google's AMIE can now interpret and reason across medical histories, lab results, and complex medical images simultaneously, and is currently being tested in clinical research settings with Beth Israel Deaconess Medical Center. Aidoc received FDA clearance in early 2025 for the first foundation model-powered clinical AI device, a rib fracture triage solution built on its CARE1™ Foundation Model. The field is moving from task-specific classifiers to systems that can support clinical reasoning at a higher level of context.
For imaging AI specifically, this matters because radiology reporting is inherently integrative. A finding on CT means something different depending on whether the patient is immunocompromised, has a history of malignancy, or just underwent a procedure. A model that reads images in isolation will always have a ceiling. A model that reads them in context has more clinical value — and more clinical responsibility.
Why Human Oversight Is Still the Right Model
The regulatory momentum behind radiology AI, and the clinical evidence for specific use cases, does not change the underlying logic: these are tools for human-guided diagnosis, not autonomous clinical judgment.
That distinction matters practically, not just philosophically. Most cleared AI systems sit in the moderate-risk category under FDA frameworks, and most are deployed with radiologists as the final interpreter. The EU AI Act, whose high-risk medical device obligations take full effect in August 2026, explicitly classifies AI-enabled medical devices as high-risk, requiring rigorous documentation of training data, bias checks, performance benchmarks, and human oversight policies. A recent npj Digital Medicine analysis walks through what these obligations mean for radiology AI providers and deployers in practice.
What this means operationally is that the most defensible AI deployments in radiology right now are the ones where the accountability chain is clear. The AI surfaces a finding. A radiologist evaluates it. The radiologist signs the report. If the AI was wrong, the radiologist's oversight is the safety net. If the AI was right and the radiologist disagreed, the radiologist's documented reasoning is the clinical record.
That is not a cumbersome workaround. It is the design principle that makes clinical AI trustworthy enough to actually use, and it aligns with the American College of Radiology's (ACR) clinical guidance on AI deployment.
A pre-deployment checklist for radiology AI
A useful checklist before deploying any radiology AI tool:
- Is the intended use narrow and clearly defined (e.g., nodule detection on chest CT, not "radiology AI")?
- Has the system been validated on data representative of your patient population and scanner hardware?
- Does the workflow keep a radiologist as the final interpreter?
- Are there mechanisms for tracking performance over time and catching distribution shift?
- Is there a clear process for handling edge cases, disagreements, and errors?
- Are privacy, data security, and HIPAA compliance addressed at the system level? The more of these boxes you can check, the more trustworthy the deployment is likely to be.
What the Next Phase of AI in Radiology Looks Like
The arc of radiology AI over the next three to five years is becoming more legible. The field is moving away from isolated detection tools and toward integrated workflow platforms that support the full reading cycle: from worklist prioritization through preliminary reporting, structured documentation, prior comparison, and follow-up flagging.
A 2026 NVIDIA survey of AI in healthcare found that 61% of medical technology organizations are already using AI for medical imaging, with medical imaging and workflow optimization ranking as the top ROI-generating use cases. That is not pilot-stage adoption — it is an industry shifting its operational baseline.
At the more ambitious end, ambient AI systems are beginning to function as persistent clinical copilots, capturing radiologist voice during the read, drafting structured reports in real time, flagging discrepancies with prior imaging, and routing urgent findings automatically. These systems do not replace the read. They reduce the administrative tax on it.
What the next generation of radiology AI will probably look like is not a smarter standalone model. It is a layer of intelligence embedded across the imaging workflow, aware of patient history, integrated with the EHR, capable of surfacing relevant priors, and able to communicate findings in plain language to referring clinicians who are not trained to interpret raw imaging reports.
That last piece — clinical communication — is where NLP and large language models have the most underappreciated role. Not as diagnostic engines, but as translators: turning the radiologist's structured findings into the clear, actionable summary that the oncologist or the emergency physician or the patient's primary care doctor actually needs.
Final Thoughts: AI in Radiology Is Infrastructure, Not Replacement
Radiology is the part of medicine that most visibly resembles a data processing problem. High-volume, image-intensive, pattern-driven, and increasingly burdened by the gap between how many scans need to be read and how many trained radiologists exist to read them.
AI in radiology does not solve that problem by replacing radiologists. It solves it by making the parts of the job that are most amenable to automation — structured pattern recognition, preliminary flagging, routine measurement, worklist prioritization — faster and more consistent, so that the radiologist's attention can go where it is hardest to replace: to the unusual case, the ambiguous finding, the patient with a complex history that does not fit the model's training distribution.
The benchmark numbers are encouraging. The regulatory trajectory is real. The production evidence is growing. But the installations that are working are not the ones that deployed AI and stepped back. They are the ones that designed AI as part of a clinical workflow, kept radiologists accountable, and treated deployment as an ongoing operational discipline rather than a one-time technology decision.
That is the right frame for this technology. Not artificial radiologists. Better radiology infrastructure. Not less human judgment. More room for judgment to be applied where it actually matters.
FAQs on AI in Radiology
Q1: Will AI replace radiologists?
No. AI in radiology is being deployed as an assistive layer, not a replacement. The FDA-cleared and EU-regulated systems available today are explicitly designed to keep a radiologist as the final interpreter. AI handles repetitive pattern recognition; the radiologist handles judgment, context, and accountability.
Q2: How accurate is AI in radiology?
Accuracy varies by task. In chest CT nodule detection, peer-reviewed studies report sensitivity up to 95%. In glioma classification on MRI, AUC values around 93% have been demonstrated. In breast cancer screening, AI has identified 25% of interval cancers missed by traditional screening. However, real-world performance can differ from benchmark performance, which is why human oversight remains essential.
Q3: Is AI in radiology FDA-approved?
Yes. As of late 2025, the FDA has authorized 1,104 AI-enabled radiology devices, representing 76% of all FDA-cleared AI medical devices. Most are cleared via the 510(k) pathway. The full list is publicly maintained on the FDA's AI/ML-enabled medical devices page.
Q4: What are the main use cases for AI in radiology today?
The most mature use cases are: (1) triage and worklist prioritization for time-critical findings like stroke or pulmonary embolism, (2) detection assistance for nodules, fractures, and lesions, (3) automated measurements and quantification, (4) structured report drafting, and (5) prior imaging comparison.
Q5: What are the limitations of AI in radiology?
Key limitations include: limited generalizability across scanner types and patient populations, potential demographic bias in training data, the gap between benchmark and real-world performance, and the relatively small percentage of approved devices with prospective clinical validation. These are the reasons human oversight is still required.
Q6: How does AI integrate with existing radiology workflows?
Modern AI tools integrate directly with PACS, RIS, and EHR systems through standards like DICOM and HL7 FHIR, often using IHE profiles. Well-designed deployments surface AI findings inside the radiologist's existing reading interface, rather than requiring a separate application.
Q7: What does the EU AI Act mean for radiology AI?
Under the EU AI Act, most AI-enabled medical devices used in radiology are classified as high-risk. The high-risk obligations entered application in August 2026 for many provisions, with full medical device CE-mark integration by August 2027. Providers must document training data, bias checks, performance, and human oversight policies.
Orydex builds AI-powered clinical imaging tools for healthcare startups, research institutions, and diagnostic teams. If you are building or evaluating radiology AI, we would be glad to talk.